Nursing home patients may find themselves subject to dozens of adverse conditions through no fault of their own: bed injuries, pressure ulcers, falls, fractures, malnutrition and dehydration are some of the more prominent injuries.
BED INJURIES
Between January 1, 1985 and January 1, 2010, the FDA received 828 incidents of patients caught, trapped, entangled, or strangled in hospital beds. The reports included 493 deaths, 141 non-fatal injuries, and 194 cases where staff needed to intervene to prevent injuries.Some side rails extend the full length of the bed; others, called half rails, are about 2-1/2 feet long and the majority can be raised or lowered. Side rails are divided, either vertically or horizontally, with slats spaced about six or more inches apart. This space can trap an elderly person’s head, creating a strangulation hazard, or allow a thin, frail person to squeeze between the rails and fall to the floor.Mattresses sometimes do no fit properly in the frame, leaving gaps large enough to trap the resident between the mattress and side rail, which can lead to suffocation. In a 2010 article published in The New York Times, Steven Miles, geriatrician and bioethicist at the University of Minnesota said, “Rails decrease your risk of falling by 10 to 15 percent, but they increase the risk of injury by about 20 percent because they change the geometry of the fall.” Bed rail guidelines and safety assessment kits can be found on the FDA website.
PRESSURE ULCERS
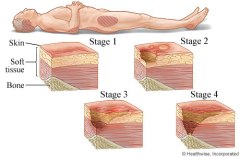
Pressure ulcers are also referred to as pressure sores, bedsores, and decubitus ulcers. A pressure ulcer can range from a very mild pink coloration to the skin, which disappears in a few hours after the pressure is relieved, to a very deep wound extending to and sometimes through a bone into internal organs. All pressure ulcers follow symptoms similar to burn wounds, ranging from mild redness (similar to a first degree burn) to a deep open wound with a blackened tissue (as a third or fourth degree burn).
The primary cause of pressure ulcers is unrelieved pressure, but can occur from friction or from prolonged exposure to cold. Any area of tissue that lies just over a bone is more likely to form a pressure ulcer. These areas include the spine, coccyx or “tailbone”, hips, heels, and elbows. Other contributing factors to the development of pressure ulcers are poor nutrition, weight loss, diabetes, poor hygiene, and dehydration.
Prevention is the most important component of pressure ulcer management. Removing all pressure from the involved areas to prevent further decay of tissue and promote healing is the primary method of treatment. Frequent turning is mandatory to alleviate pressure on the wound and to promote healing. The individual must have increased nutrition to allow for proper healing of the wounds.
Another key aspect of treatment is keeping the area clean and removing dead or necrotic tissue which can form a breeding ground for infection. Some deep wounds require surgical removal, called debridement, of dead tissue. Without all of these elements being in place the wounds will not heal properly and will likely worsen.
Pressure ulcers may indicate potential problems with the care being delivered to the nursing home resident. Even in good nursing homes, small wounds may develop, but with attention, these wounds will heal. According to Federal law, in most situations there is no medically valid reason for a pressure ulcer to progress to a Stage IV situation (a massive deep open wound).
FALLS AND FRACTURES
Falls are the most frequent cause of fractures in the elderly. Nursing home residents are at increased risk of falls due to their age, but there are other factors as well. Nursing home personnel are required to assess patients regularly to determine their risk for falling and provide safety devices and services to minimize the risk of injury to the resident. Some of the risk factors for falls include:
Previous falls
Cardiac arrhythmias
Stroke
Central nervous system disorders such as Alzheimer’s disease, Parkinson’s disease, dementia and others
Problems with mobility and gait
Low blood pressure (orthostatic hypotension) on standing up
Bowel or bladder incontinence
Dizziness
Dehydration
Visual impairment
Use of restraints
Medications
MALNUTRITION
Nutritional well-being is an important part of successful aging. Improper nutrition or malnutrition can lead to infections, confusion, and muscle weakness resulting in immobility and falls, pressure ulcers, pneumonia, and decreased immunity to bacteria and viruses. Malnutrition is costly, lowers the quality of life of the nursing home resident and is often avoidable. The facility must take steps to ensure that residents maintain good nutritional health and must provide residents with well-balanced, palatable meals.
Many things can cause malnutrition in nursing home residents. The following are factors that may prevent a resident from receiving adequate nutritional needs:
Physical Causes:
Illness
Adverse drug effects such as nausea, vomiting, diarrhea, cognitive disturbances or sleepiness
Food and drug interactions which decrease the ability of the body to absorb vitamins and minerals
Depression
Swallowing disorders
Mouth problems such as tooth loss, dentures that do not fit properly, mouth sores, and mouth pain
Tremors, which affect the residents’ ability to feed themselves
Environmental Causes:
Inadequate attention from staff for residents who need assistance eating
Staff who are uneducated about malnutrition and proper ways to feed residents who need help
Reliance on liquid supplements
Special diets
Signs That a Resident is Malnourished
Do clothes fit more loosely than usual?
Are there cracks around the mouth?
Do lips and mouth look pale?
Has the resident complained that his/her dentures no longer fit?
Has the resident’s hair been thinning or growing sparse?
Do wounds seem to take longer to heal?
Does the resident appear confused (not as a result of a disease such as Alzheimer’s)?
Is the resident’s skin breaking down?
Do the resident’s eyes look sunken?
Does the resident appear to be losing weight?
If the answer is yes to two or more of these questions, the following may help pinpoint specific problems:
Can the resident feed him/herself?
What is the resident’s favorite meal of the day?
When and where does the resident prefer to have meals served?
Does it take a long time for the resident to eat?
Is the resident rushed through meals?
Is the resident unable to finish meals?
Does the resident seem to eat more when someone is there to help with the meal?
Does the resident seem uninterested in food?
Has the resident lost his/her appetite?
Does the resident like the food at the facility?
Can the resident choose from a menu?
Are snacks readily available to the resident?
Is the resident on a special diet?
Has the resident started taking any new medications?
Has the resident’s weight routinely been monitored?
Has the staff informed family members of weight loss?
Has staff asked family members for assistance?
DEHYDRATION
Dehydration should be managed through an individualized daily plan to promote adequate hydration based upon identifying the risk factors which include at least the following:
Alzheimer’s, or other dementia
Major psychiatric disorders
Depression
Stroke
Repeated infections
Diabetes
Malnutrition
Urinary incontinence
History of dehydration
4 or more chronic conditions
Use of diuretics, antidepressants, psychotropics, or anti-anxiety medications, laxatives, or steroids
SPMH Law, LLC represents clients throughout Georgia and the Southeastern United States. To schedule a free consultation with a lawyer at our firm, call us at 404-882-5115 or visit us online at www.eldercareabuselawyer.com.
Serving clients in:
Atlanta, Bartow, Cherokee, Cobb, Floyd, Fulton, Whitfield, Douglas, Polk, Chatham and all of Northwest Georgia, North Georgia, Central Georgia and South Georgia, as well as much of the Southeastern United States.
 Between January 1, 1985 and January 1, 2010, the FDA received 828 incidents of patients caught, trapped, entangled, or strangled in hospital beds. The reports included 493 deaths, 141 non-fatal injuries, and 194 cases where staff needed to intervene to prevent injuries.Some side rails extend the full length of the bed; others, called half rails, are about 2-1/2 feet long and the majority can be raised or lowered. Side rails are divided, either vertically or horizontally, with slats spaced about six or more inches apart. This space can trap an elderly person’s head, creating a strangulation hazard, or allow a thin, frail person to squeeze between the rails and fall to the floor.Mattresses sometimes do no fit properly in the frame, leaving gaps large enough to trap the resident between the mattress and side rail, which can lead to suffocation. In a 2010 article published in The New York Times, Steven Miles, geriatrician and bioethicist at the University of Minnesota said, “Rails decrease your risk of falling by 10 to 15 percent, but they increase the risk of injury by about 20 percent because they change the geometry of the fall.” Bed rail guidelines and safety assessment kits can be found on the FDA website.
Between January 1, 1985 and January 1, 2010, the FDA received 828 incidents of patients caught, trapped, entangled, or strangled in hospital beds. The reports included 493 deaths, 141 non-fatal injuries, and 194 cases where staff needed to intervene to prevent injuries.Some side rails extend the full length of the bed; others, called half rails, are about 2-1/2 feet long and the majority can be raised or lowered. Side rails are divided, either vertically or horizontally, with slats spaced about six or more inches apart. This space can trap an elderly person’s head, creating a strangulation hazard, or allow a thin, frail person to squeeze between the rails and fall to the floor.Mattresses sometimes do no fit properly in the frame, leaving gaps large enough to trap the resident between the mattress and side rail, which can lead to suffocation. In a 2010 article published in The New York Times, Steven Miles, geriatrician and bioethicist at the University of Minnesota said, “Rails decrease your risk of falling by 10 to 15 percent, but they increase the risk of injury by about 20 percent because they change the geometry of the fall.” Bed rail guidelines and safety assessment kits can be found on the FDA website.
 Pressure ulcers are also referred to as pressure sores, bedsores, and decubitus ulcers. A pressure ulcer can range from a very mild pink coloration to the skin, which disappears in a few hours after the pressure is relieved, to a very deep wound extending to and sometimes through a bone into internal organs. All pressure ulcers follow symptoms similar to burn wounds, ranging from mild redness (similar to a first degree burn) to a deep open wound with a blackened tissue (as a third or fourth degree burn).
The primary cause of pressure ulcers is unrelieved pressure, but can occur from friction or from prolonged exposure to cold. Any area of tissue that lies just over a bone is more likely to form a pressure ulcer. These areas include the spine, coccyx or “tailbone”, hips, heels, and elbows. Other contributing factors to the development of pressure ulcers are poor nutrition, weight loss, diabetes, poor hygiene, and dehydration.
Prevention is the most important component of pressure ulcer management. Removing all pressure from the involved areas to prevent further decay of tissue and promote healing is the primary method of treatment. Frequent turning is mandatory to alleviate pressure on the wound and to promote healing. The individual must have increased nutrition to allow for proper healing of the wounds.
Another key aspect of treatment is keeping the area clean and removing dead or necrotic tissue which can form a breeding ground for infection. Some deep wounds require surgical removal, called debridement, of dead tissue. Without all of these elements being in place the wounds will not heal properly and will likely worsen.
Pressure ulcers may indicate potential problems with the care being delivered to the nursing home resident. Even in good nursing homes, small wounds may develop, but with attention, these wounds will heal. According to Federal law, in most situations there is no medically valid reason for a pressure ulcer to progress to a Stage IV situation (a massive deep open wound).
Pressure ulcers are also referred to as pressure sores, bedsores, and decubitus ulcers. A pressure ulcer can range from a very mild pink coloration to the skin, which disappears in a few hours after the pressure is relieved, to a very deep wound extending to and sometimes through a bone into internal organs. All pressure ulcers follow symptoms similar to burn wounds, ranging from mild redness (similar to a first degree burn) to a deep open wound with a blackened tissue (as a third or fourth degree burn).
The primary cause of pressure ulcers is unrelieved pressure, but can occur from friction or from prolonged exposure to cold. Any area of tissue that lies just over a bone is more likely to form a pressure ulcer. These areas include the spine, coccyx or “tailbone”, hips, heels, and elbows. Other contributing factors to the development of pressure ulcers are poor nutrition, weight loss, diabetes, poor hygiene, and dehydration.
Prevention is the most important component of pressure ulcer management. Removing all pressure from the involved areas to prevent further decay of tissue and promote healing is the primary method of treatment. Frequent turning is mandatory to alleviate pressure on the wound and to promote healing. The individual must have increased nutrition to allow for proper healing of the wounds.
Another key aspect of treatment is keeping the area clean and removing dead or necrotic tissue which can form a breeding ground for infection. Some deep wounds require surgical removal, called debridement, of dead tissue. Without all of these elements being in place the wounds will not heal properly and will likely worsen.
Pressure ulcers may indicate potential problems with the care being delivered to the nursing home resident. Even in good nursing homes, small wounds may develop, but with attention, these wounds will heal. According to Federal law, in most situations there is no medically valid reason for a pressure ulcer to progress to a Stage IV situation (a massive deep open wound).
 Falls are the most frequent cause of fractures in the elderly. Nursing home residents are at increased risk of falls due to their age, but there are other factors as well. Nursing home personnel are required to assess patients regularly to determine their risk for falling and provide safety devices and services to minimize the risk of injury to the resident. Some of the risk factors for falls include:
Falls are the most frequent cause of fractures in the elderly. Nursing home residents are at increased risk of falls due to their age, but there are other factors as well. Nursing home personnel are required to assess patients regularly to determine their risk for falling and provide safety devices and services to minimize the risk of injury to the resident. Some of the risk factors for falls include:
 Dehydration should be managed through an individualized daily plan to promote adequate hydration based upon identifying the risk factors which include at least the following:
Dehydration should be managed through an individualized daily plan to promote adequate hydration based upon identifying the risk factors which include at least the following: